Confusion Results in Freight Train Incident, New South Wales (Bad Day)
Unclear communication, confusion, and misunderstanding led to a freight train incident in New South Wales.
It happened shortly after midnight on August 12, 2019, near Waterfall, NSW, as noted by ATSB (Australian Transport Safety Bureau): Unclear communication, confusion, and misunderstanding of safe working network rules resulted in a safe working irregularity involving a freight train driver who unknowingly entered the track without protections.
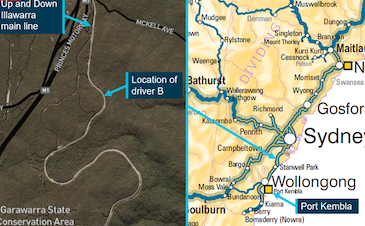
The freight train incident occurred while a driver was manually releasing hand brakes on Pacific National freight train 4WM2 following a remarshal* of the train consist to clear the main line due to a track fault on the adjoining network that prevented the train from travelling past signal W26U.
The remarshal involved dividing the train’s three locomotives from its rake of 50 wagons and manually securing the wagons’ hand brakes on the Up direction on the Up line near the signal. The locomotives then traveled to Helensburgh for a return journey toward Waterfall on the Up direction on the Up line to reattach the stabled wagons.
On arrival at the wagons, one of the two drivers from 4WM2 requested protections be put in place before entering the track on the Down line to reattach the locomotives and release the wagon hand brakes. During this time, a passenger train was diverted from the Up line to travel in the Up direction on the Down line to Waterfall to avoid the freight train.
As the driver released the hand brakes, the second driver on 4WM2 saw a passenger train approaching the driver on the Down line and signalled for the train to stop. The passenger train made an emergency brake application to stop before reaching the driver. There were no injuries.
A transport safety investigation into the incident conducted by the Office of Transport Safety Investigations, which undertakes rail safety investigations in New South Wales on behalf of the ATSB, established that the safeworking network rule and procedure for protecting activities associated with in-service rail traffic were not used effectively to ensure workers were protected from rail traffic.
The requests for protection were informal and did not detail the required activities or protection, the investigation notes. Both drivers of 4WM2 unknowingly entered the danger zone without appropriate protection and were at risk of being struck by rail traffic.
There were multiple parties involved in the communication and decision making relating to the movements of 4WM2, the investigation found. This led to confusion and misunderstanding of the required activities and likely affected the actions of the Waterfall Signaller and train crew. Additionally, not all communications were conducted in accordance with the network rules.
“Key lessons from this investigation are that rail infrastructure managers and rail transport operators must ensure that safety critical communication is conducted in accordance with network rules and that network controllers consider the potential dangers train crews are exposed to before requiring them to enter the danger zone, as part of a broader system to ensure the safety of workers entering the danger zone,” said OTSI Chief Investigator Dr. Natalie Pelham.
“Workers must also ensure they have appropriate safeworking protection in place before entering the danger zone to protect them from rail traffic. Additionally, workers must ensure rest periods are utilised to manage non-work-related fatigue to complement rail infrastructure managers and rail transport operators’ fatigue management programs,” said Dr. Pelham.
The rail operator and network owner have taken several proactive safety actions as result of the incident.
*Remarshal refers to changing the order of locomotives or wagons in a train consist.
Through TapRooT® RCA Training, we can help your management understand how advanced root cause analysis works and how it can help your site/company achieve excellence.
It starts with a FREE executive briefing. Visit our Executive Portal to request a free, 1-hour Executive Briefing. TapRooT® Root Cause Analysis was developed to meet the proven requirements for systematic root cause analysis. We can help you implement the proven TapRooT® process, and we will work with you to develop your custom plan.
Register for a TapRooT® Root Cause Analysis Training Course.
TapRooT® Root Cause Analysis Training courses are taught all over the world. If you are interested in learning how to stop repeat incidents, find a 2-day or 5-day course. We are available to train you and your staff on-site at your workplace; contact us to discuss your needs. You may also call us at 865.539.2139.