Thinking Fast: Pilot Errors & Causal Factors in Unstabilized Approaches
If an unstabilized approach is continued, aircraft damage, destruction, personal injury, or death could result.
Aviation approaches become unstabilized for many reasons. Causes include adverse weather, ATC instructions, runway changes, schedule pressure, and human factors. Today, we’re looking at four reports of unstabilized approaches and unintended consequences that were sparked and allowed to develop primarily due to human factors.

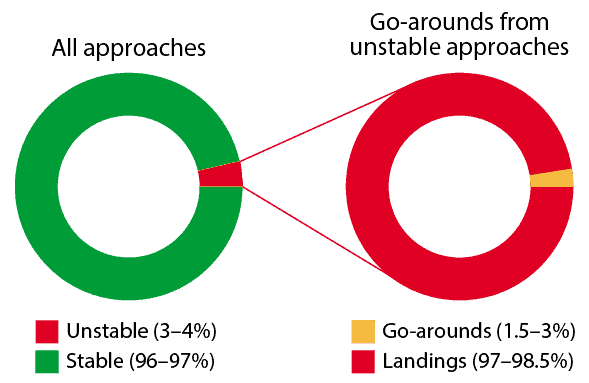
The stabilized approach has long been promoted by the FAA, safety organizations, and most airlines as the standard of flight performance that must be maintained throughout an approach in order to continue to minimums. Key elements of a stabilized approach are described in the FAA Airplane Flying Handbook. The airplane should be in the landing configuration early in the approach with the landing gear down, planned landing flaps selected, trim set, and fuel balanced. The aircraft should be on profile before descending below 1,000 feet AGL, and an optimum glidepath of 2.5 to 3.0 degrees established and maintained. Indicated airspeed should be within 10 knots of target airspeed, and descent rate 500 to 700 FPM, not to exceed 1,000 FPM. Engine RPM should allow the best response if a rapid power increase is needed. If any of these tolerances are exceeded during an approach, the approach is unstabilized, unsafe, and must be abandoned.
Anticipating MEL consequences
The unanticipated consequences of an MEL (Minimum Equipment List; meaning a particular aircraft appliance is broken but is not needed for safe flight) item magnified the effect of a late descent clearance for an ERJ-145 Captain. The approach was unstabilized, and the situation worsened.
Here is his account of the experience.
■ This was our first flight of the day in this airplane. The airplane had an MEL on the engine anti-ice valve, which required the anti-ice to be on for the duration of the flight. I was the Pilot Monitoring (PM). . . . We found out very quickly on the arrival into IAD (Dulles International Airport) that the airplane was going to create challenges making crossing restrictions. With the anti-ice on, the thrust would not drop below 55% N1, which is normal when anti-ice is on, but makes it very difficult to descend and slow. . . . We applied speed brakes to assist in slowing, but it still didn’t help enough. A late descent clearance for the ILS (Instrument Landing System) . . . complicated things, and we were too fast and not configured by the Final Approach Fix (FAF) in IMC (Instrument meteorological conditions) with weather lower than visual minimums. I called for the missed approach, and the PF (Pilot Flying) . . . arrested the descent. I advised Tower that we were going missed, and the instruction was to follow the localizer inbound and climb to 2,000 feet. During the clearance I realized that TOGA (Takeoff/Go-around switch) had not been selected yet, so I selected TOGA to bring the FD (Flight Director) up. I asked Tower for higher as we were already above 2,000 feet when the clearance was [issued]. The published missed was 3,000 feet. Tower cleared us for 4,000 feet. Sometime during this exchange the PF had disconnected the autopilot. The airplane began rolling right. I assisted the PF on the controls to arrest the roll and work back toward the localizer, which at this time . . . was full scale deflection to the left. We received a clearance for runway heading, continued the climb to 4,000 feet, and proceeded with checklists and . . . a normal landing.
During debrief, the PF was unaware that he had disconnected the autopilot. It was this inadvertent disconnect that led to the aircraft rolling right off course. The autopilot should have been used for the missed [approach]. Turning the autopilot off greatly increased the workload, causing the momentary loss of situational awareness. The MEL applied to the airplane created an increased workload on every leg we flew this airplane . . . [that] day.
CRM over and over
An air carrier First Officer misidentified a ground reference during a charted visual approach. No comment or suggestion was offered by the Pilot Monitoring (PM), and the result was an unstabilized approach.
Let’s hear what happened:
■ I was the Pilot Flying (PF) for the flight into PWM. Approaching the airport, we were assigned the Harbor Visual to Runway 29. We crossed the coast eastbound at . . . 3,000 feet and made a left, northbound turn toward the islands. We had previously briefed the approach. . . . The Captain and I were trying to identify the lighthouses and islands that we were supposed to turn between.
I called out two islands that I believed to be the two to turn between. The Captain concurred. I selected pattern altitude of 1,500 feet and began a manual descent with the Flight Director (FD) on. Slowing the aircraft early to prevent coming in too fast on this visual, we were flying . . . 180 knots in the descent. We overflew an island, and the Captain announced, “You need to turn hard, now.” Apparently, the islands that I had identified were not the same that he understood.
I began a . . . left turn to join the harbor. In this confusion, I did a poor job monitoring my altitude. Both of us forgot to continue configuring the aircraft. At 1,000 feet AGL (above ground level), we received a chime denoting that the gear is not down. The Captain instructed, “Level off.” While still in the left turn, I pitched the nose up and added a slight power increase. We configured the aircraft in the next few seconds and continued our descent at Vref+5. (approach speed) The aircraft landed successfully.
The poor communication between the Captain and myself led to this event. We had experienced similar poor communication [during] this pairing. It is my belief that the Captain knew when to turn, but failed to correct my island identification, due to his comment of flying this . . . approach “many times.” The [failure] to confirm the turn inbound led to a distraction, which led to an unstabilized approach.
The approach should have ended as soon as we realized that we were off course and behind the aircraft. . . . My hesitation with calling the go-around comes from being a low-time First Officer flying this approach for the first time and having an extremely experienced Captain in the left seat. His reassurance that these deviations were okay to land led me to not go around.
Universal risks
This flight crew experienced several common risk factors. Failure to mitigate the threats resulted in an unstabilized approach, rife with wisdom for all aviators.
From the Captain’s report:
■ I was flying my second Captain trip, and I was practicing [an] HGS CAT III Approach. Inexperience is definitely a risk factor. . . . The weather was calm and clear. Somewhere around the FAF, I became distracted and forgot to call for final flaps 30 and the landing checklist. I allowed myself to become completely engrossed by the procedures and callouts. Distraction was the second risk factor. Somewhere below the 500 foot callout, I heard, “TOO LOW FLAPS.” I looked at the flap indicator and saw that the flaps were still at 15. I immediately called for flaps 30 [and the landing] checklist. The First Officer complied, and by the time we had completed the checklist, the radio altimeter was making the [altitude] callouts. Things happened so fast that I did not think to go around. Being rushed was the third risk factor. I landed, and realized on landing rollout that “TOO LOW FLAPS” is not a caution, but a warning. I was in violation of go-around/missed approach requirements.
From the First Officer’s report:
■ During final approach as PM, I failed to recognize that we were not properly configured from flaps 15 to flaps 30 for landing. . . . During the final approach segment, I became internally distracted, trying to simulate as best as possible the CAT III conditions, as it has been some time since I have conducted those procedures. I [incorrectly] made the . . . mode callout at the FAF. Additionally, I was trying to remember . . . thrust lever [procedures]. This distraction caused a lack of situational awareness and a lack of proper configuration. Somewhere below 400 feet AGL, we got the “TOO LOW FLAPS” auditory warning and immediately recognized our error. The Captain called for flaps 30 and the landing checklist, which I complied with. We made an uneventful landing. In retrospect, I should have called for the go-around upon hearing the auditory warning for flap configuration.
Routine changes that aren’t
An Airbus Captain was dismayed at the mistake that led to this unstabilized approach. Unrecognized fatigue, always insidious, was identified as a contributing factor.
What else can you find that contributed to the unstabilized approach?
■ At the end of a long duty day, I felt capable. . . . I had 9 hours of sleep the night before and felt rested. We took off 25 minutes before our out-of-duty time due to maintenance issues. . . . At no time did I feel fatigued during this flight but, looking back, fatigue played a part in this problem.
The point that I normally would configure is when we were offered the runway change. I then directed the First Officer to disregard attempting to load the runway change into the Flight Management Guidance Computer (FMGC) and told him I would fly the approach visually. I knew that the center runway touchdown zone was closer to me than the left runway touchdown zone, and I began to descend at a more rapid rate to make the Precision Approach Path Indicator (PAPI) look correct. My attention was channelized on the acquisition of the proper glide path of the new runway. I really felt I was doing a great job at this until the Master Caution and associated warning bells began to ring around 600 feet. I immediately knew what I had done wrong and began the go-around. The airplane configuration at the point of the Master Caution was only Flaps 2 with gear up. I can honestly say that if not for this gear warning system, tonight I would have landed gear up. I was so concentrated on making this runway change and landing that I forgot to properly configure the aircraft. The go-around was expertly assisted by the First Officer. I needed the help to ensure proper aircraft operation because I was stuck back at the point of the error in disbelief that I could do something that stupid. The go-around was eventually executed properly, and the following landing was normal and uneventful. Fatigue was unrecognized tonight but played a factor, since I would have been able to direct the proper configuration had this been the first flight of the day.
The above narratives originate with CALLBACK, NASA’s Aviation Safety Reporting System (ASRS). ASRS captures confidential reports, analyzes the resulting aviation safety data, and disseminates vital information to the aviation community.
The TapRooT® System trains you to solve problems
Circumstances can crop up anywhere at any time if proper and safe sequence and procedures are not planned and followed. We encourage you to learn and use the TapRooT® System to solve problems.
TapRooT® has a team of investigators and instructors with years of extensive training ready to offer assistance worldwide. We also offer ongoing support to our clients through free newsletters and Root Cause Tip Videos, the Root Cause Analysis Blog, and our annual Global TapRooT® Summit.
Register for a TapRooT® Course
Register for one of our Courses. We offer a basic 2-Day Course and an advanced 5-Day Course.
Contact us, or call 865.539.2139 about having a course at your site or for further root cause analysis training opportunities. We’re here to find solutions for you.